Enhanced equine clinical arbovirus surveillance project — final results
Karen Moore
Senior Surveillance Officer (Epidemiology)
In response to flooding across Victoria in 2016, the Department of Health and Human Services (DHHS) provided funding for the investigation of clinical signs typical of mosquito-borne arboviral infection in Victorian horses.
The aims of the project were to:
- estimate the total incidence of Murray Valley encephalitis virus (MVEV), Ross River virus (RRV) and West Nile virus (Kunjin strain) (WNV/KUN) as the cause of neurological signs in Victorian horses in the period immediately after the 2016 floods
- evaluate the use of data from clinically affected horses as a source of passive surveillance for RRV and MVEV in humans, through assessment of the correlation between human and equine cases, by region and over time.
Free laboratory testing and veterinary subsidies were provided for disease investigation of horses with neurological or muscular signs consistent with an arboviral infection. Samples were tested for flavivirus, RRV and Hendra (a differential diagnosis for horses showing neurological signs). An initial and convalescent blood sample (2 to 3 weeks later) were collected to determine the true RRV status of the animals (current infection, historic infection or non-infection).
Results
The project received initial samples from 85 horses (80 individual properties) between 1 February 2017 and 13 June 2017.
Convalescent samples were also received from all but 8 horses. Study horses were located throughout the state (Figure 1), with the exception of the far north-western region. Thirty-seven veterinary practices undertook investigations for the project.
Figure 1. Geographic distribution across Victoria of study horses with clinical signs typical of infection with an arbovirus, sampled between 8 February 2017 and 13 June 2017
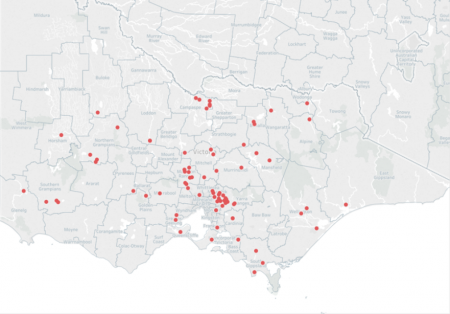
Map of Victoria that shows the number of investigations in each shire were: Benalla 3, Buloke 1, Campaspe 6, Cardinia 2, Casey 1, East Gippsland 1, Glenelg 1, Golden Plains 1, Greater Geelong 3, Horsham 1, Hume 1, Indigo 1, Knox 1, Loddon 2, Macedon Ranges 9, Manningham 2, Mansfield 2, Mitchell 4, Moorabool 1, Mornington Peninsula 1, Murrindindi 2, Nillumbik 6, Northern Grampians 4, Pyrenees 1, South gippsland 4, Southern grampians 3, Strathbogie 1, Wangaratta 1, Wellington 3 and Yarra Ranges 16
Hendra virus
All samples tested negative for Hendra virus.
Ross River virus (RRV)
Seven horses were identified with antibody titres consistent with recent infection with RRV. RRV could not be confirmed or excluded (results were inconclusive) for 16 horses and 53 had no evidence of recent infection.
Confirmed RRV cases were sampled between 11 February and 15 March (Figure 2).
Figure 2. Number of study horses (n=85) investigated (grey) and, of these, number confirmed to be infected recently with Ross River virus (RRV positive) (black)
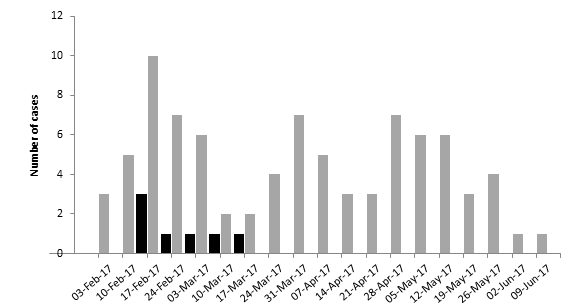
7 positive cases of Ross River virus were confirmed between 11 February and 15 March 2017. Investigations continued until 9 June 2017 with no other positive cases.
Horses with confirmed RRV infection and inconclusive RRV results were distributed throughout the state (Figure 3). There was no obvious geographic localisation of cases.
Figure 3. Geographic location of study horses within Victoria diagnosed with a conclusive (positive) or inconclusive result on serological testing for Ross River virus between 8 February 2017 and 13 June 2017.
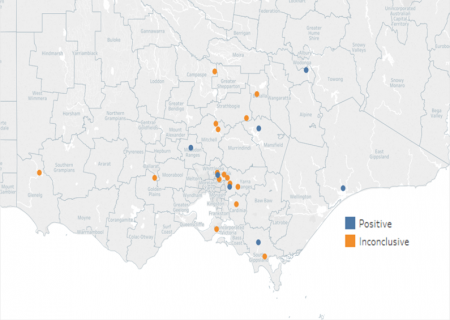
The shires each had one positive Ross River virus case: Mansfield, East Gippsland, Indigo, Macedon ranges Nillumbik, South Gippsland and the Yarra Ranges. Shires with one inconclusive results were Benalla, Campaspe. Cardinia, Glenelg, Golden Plains,Mornington Peninsula, South Gippsland, Strathbogie. Mitchell shire had 2 inconclusive results and Nillumbik had 3 inconclusive results
Murray Valley encephalitis virus (MVEV)
Although three horses initially tested positive to MVEV antibodies, in all cases, the antibodies were indicative of a historic infection.
These horses were located in the local government areas (LGAs) of Yarra Ranges and Northern Grampians at the time of sampling.
West Nile virus – Kunjin subtype (WNV/KUN)
Although two horses had antibodies to WNV/KUN, the detected antibodies were indicative of a historic infection.
Affected horses were located in the LGAs of Campaspe and Nillumbik at the time of sampling.
Incidental flaviviruses
Seven horses were diagnosed with incidental flavivirus antibodies (meaning, flavivirus-positive but test-negative to MVE and WNV/KUN). These incidental flaviviruses were considered likely to be non-pathogenic.
Clinical signs
The most commonly reported clinical signs for horses without confirmed RRV infection were an altered mental state, ataxia, oedema, lameness and pyrexia (Table 1).
The most common clinical sign(s) for horses with confirmed RRV infection were very similar:
- altered mental state
- oedema
- pyrexia
- ataxia.
This indicates that arboviral infection may not be differentiated based solely on clinical observation in Victorian horses.
Table 1. Clinical signs observed in Victorian study horses with (n=7) and without (n=78) a confirmed, recent Ross River virus (RRV) infection
Note: Multiple signs could be selected for each case
| Clinical signs | RRV-negative or inconclusive cases (% of number reported) | RRV-confirmed cases (% of number reported) |
|---|---|---|
Altered mental state | 54 (69.2%) | 5 (71.4%) |
Ataxia | 26 (33.3%) | 2 (28.5%) |
Oedema | 22 (28.2%) | 5 (71.4%) |
Lameness | 22 (28.2%) | 1 (14.3%) |
Pyrexia | 18 (23.1%) | 4 (57.1%) |
Weight loss | 15 (19.2%) | 1 (14.3%) |
Muscle fasciculations | 12 (15.4%) | 1 (14.3%) |
Reluctance to walk | 11 (14.1%) | 1 (14.3%) |
Gastrointestinal signs | 12 (15.4%) | 0 (0.0%) |
Lethargic | 10 (12.8%) | 0 (0.0%) |
Recumbency | 9 (11.5%) | 0 (0.0%) |
Inappetance | 8 (10.3%) | 0 (0.0%) |
Hypermetria | 7 (9.0%) | 1 (14.3%) |
Hyperaesthesia | 7 (9.0%) | 2 (28.5%) |
High fibrin | 3 (3.8%) | 0 (0.0%) |
Respiratory signs | 3 (3.8%) | 0 (0.0%) |
Seizures | 2 (2.6%) | 0 (0.0%) |
Tachycardia | 2 (2.6%) | 0 (0.0%) |
Poor performance | 2 (2.6%) | 0 (0.0%) |
Anaemia | 2 (2.6%) | 0 (0.0%) |
Back arching | 0 (0.0%) | 1 (14.3%) |
Blindness | 0 (0.0%) | 1 (14.3%) |
Painful coronary bands | 0 (0.0%) | 1 (14.3%) |
Congested mucous membranes | 1 (1.3%) | 0 (0.0%) |
Facial paralysis | 1 (1.3%) | 0 (0.0%) |
Jaundice | 1 (1.3%) | 0 (0.0%) |
Muscle wastage | 1 (1.3%) | 0 (0.0%) |
Poor coat | 1 (1.3%) | 0 (0.0%) |
With the exception of 2011, which was the year of the previous outbreak of clinical arboviral infections in Victorian horses, the number of submissions for this project alone was approximately equivalent to the highest annual number of horse submissions received in any previous year since data collection began. There was a reasonable geographic spread of investigations across Victoria, indicating that the project information was well disseminated to practices. Despite this, there was a lack of submissions from the far north-west region of the state (the LGAs of Mildura, Swan Hill and Gannawarra).
Confirmed or likely RRV infection was found in significantly fewer horses relative to the 2011 outbreak, where there were more than 470 equine cases recorded. Despite high mosquito numbers and climatic conditions resulting in an outbreak of RRV in the human population, conditions this season do not appear to have been conducive to the development of widespread equine arboviral infection. It would seem that there may be a fundamental difference in the conditions this season compared to the 2010 to 2011 season that led to the outbreak of RRV in horses.
Currently, an adjunct project is being undertaken to determine the final diagnosis for those horses with clinical signs typical of arboviral infection, but negative for recent infection with RRV, MVEV and WNV/KUN, to enable the refinement of the current list of clinical signs thought to be associated with infection with clinical arboviral infections.
Note: As a result of this study, we have modified the Significant Disease Investigation program and will now provide a supplementary subsidy to veterinarians for the collection of an additional, convalescent blood sample from horses with suspected arboviral infections.
We will be also be working with the DHHS to further investigate the usefulness of horses as a passive surveillance method to augment current human arbovirus surveillance programs.
Read more about arboviral infection in horses.